A woman in her 40s living in Sakuragicho complained of pain when raising her left shoulder.
Clinical Case: Shoulder Pain on Elevation (Onset Without Trauma)
Approximately two weeks ago, the patient began experiencing a catching or impingement-like pain when raising her left shoulder. The discomfort initially began as a vague sensation while putting on clothes, but has since progressed to the point where pain is now felt at certain angles during shoulder elevation.
There was no identifiable cause or incident that triggered the onset, and she reported that the pain “just started without warning.” She visited a hospital last week and had an X-ray taken, which showed no abnormalities. However, as the only treatment offered was painkillers and topical patches, she began to feel uneasy about the lack of a clear explanation. Having previously visited my chiropractic clinic for low back pain, she decided to return to seek care for this new issue.
[Initial Symptoms]
- Interview:
The frequency of the pain has been increasing, and the patient now experiences discomfort during daily activities such as putting on clothes or reaching for the overhead handrails on a train. As a result, she is growing increasingly anxious about the possibility of the condition worsening in the future.
The pain is localized to a specific area and does not occur during other arm movements, such as swinging the arm—only when raising the shoulder.
- Visual Inspection:
Visual assessment revealed no notable abnormalities.
- Static Palpation:
Palpation of the superficial layers (light pressure) revealed mild hypertonicity in the left deltoid region.
Marked tension was observed in the rotator cuff muscles attaching from the scapula to the shoulder joint.
Additionally, the muscles connecting the scapula to the spine also showed increased tension on the left side.
- Motion Palpation:
Active Range of Motion (patient lifts arm voluntarily): Pain is present when lifting the arm slightly above shoulder level (approximately 90 degrees), but the pain subsides beyond that range, and there is no discomfort at full elevation.
Passive Range of Motion (practitioner moves the relaxed arm): Mild discomfort is noted in the same range, but the intensity is significantly less compared to active movement.
- Orthopedic Tests:
Painful Arc: Positive (+)
Drop Arm Test: Negative (–)
Codman’s Test: Positive (+), indicating supraspinatus tendon pain
All of the above tests were performed to assess for possible impingement syndrome, with a focus on evaluating the supraspinatus tendon.
The Yergason’s and Speed’s tests were not performed, as the pain location differs from that typically associated with biceps tendon pathology, which these tests are intended to assess.
- Muscle Strength Examination:
Only the supraspinatus muscle strength test was performed, and no decrease in muscle strength or pain was observed in the test position.
[Initial Treatment Plan]
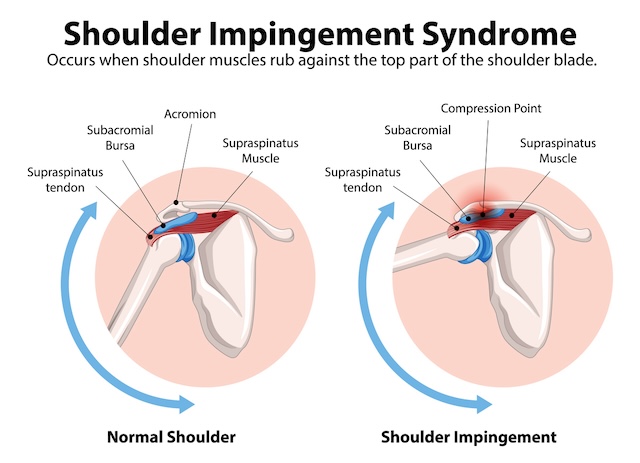
I diagnosed the condition as a straightforward case of shoulder impingement syndrome, without inflammation (like calcific tendinitis or subacromial bursitis) or joint adhesions, and created a treatment plan based on that.
First Treatment Session:
My main focus was to improve the movement of the shoulder blade—not just by working on the supraspinatus muscle (which was getting pinched), but also by releasing the tension around the muscles surrounding the scapula.
Muscle Work:
I worked on the rotator cuff muscles (supraspinatus, infraspinatus, subscapularis, teres minor—these connect the shoulder blade to the upper arm), as well as other key muscles like the rhomboids (connecting the scapula to the spine), levator scapulae (connecting the scapula to the neck), pectoralis major and minor, deltoid, biceps, and triceps.
Since these muscles all play a big role in arm movement, I focused on relaxing them to reduce strain on the shoulder joint.
Joint Work:
Her shoulder was rotated inward (internally rotated), which was putting stress on the back part of the supraspinatus tendon. So I used a joint mobilization technique to help guide the shoulder into more external rotation.
I also corrected a slight misalignment in her 5th and 6th ribs on the left side, which were pushing up the shoulder blade and causing it to wing outward. I used an adjustment to fix that.
Since her work schedule only allows to come in on weekends, I recommended a follow-up visit on Sunday, one week later.
[Prognosis]
Second Visit:
By the time she came in for her second visit, most of the pain was already gone, and there hadn’t been any noticeable change in pain even after a full week.
I continued with the same type of treatment as before, but this time I also included some work on her lower back — partly as a preventative measure, since I had treated that area in the past.
I recommended the next visit in two weeks, just to monitor progress.
Third Visit:
She came back two weeks later, and since the pain was completely gone, I decided to wrap up the treatment.
Since then, at her request, we’ve been doing full-body maintenance sessions once a month — and we’re now into the second year of that routine.
[Practitioner’s Opinion]
Before coming to Spine chiropractic, this person had already gone to an orthopedic clinic and had an X-ray done, which showed no abnormalities. So, based on that, I assumed that it hadn’t progressed into calcific tendonitis (calcium buildup in the supraspinatus tendon).
Since the issue seemed to be a straightforward case of the tendon getting pinched (without inflammation or other complications), the treatment wasn’t particularly difficult.
She also came in just two weeks after the symptoms started, which made it possible to improve things early on.
If shoulder impingement progresses, it can lead to tendonitis or bursitis, and in some cases, inflammation can cause the joint to become stuck (adhesions). When that happens, it can take months to a year before the arm can lift above 90° again.
Luckily, this person had seen me before for lower back pain (which improved and was resolved), so she already knew what to expect from my chiropractic treatment. That familiarity likely encouraged her to come in early this time — and that early visit made a big difference in her quick recovery.
At Spine Chiropractic, I address a wide range of musculoskeletal conditions directly impacting daily life, not merely as a form of relaxation therapy. Conveniently located within a one-minute walk from Bashamichi Station, an eight-minute walk from Nihon-Odori Station, a seven-minute walk from JR Kannai Station, and a 12-minute walk from JR Sakuragicho Station, my clinic is well-suited for residents and workers in the Yokohama area.
If you are experiencing similar symptoms, please feel free to visit Spine Chiropractic. I am committed to providing care with sincerity and professionalism.